
Description
Impingement is one of the most common causes of pain in the adult shoulder. It results from pressure on the rotator cuff from part of the shoulder blade (scapula) as the arm is lifted.
The rotator cuff is a tendon linking four muscles – the supraspinatus, the infraspinatus, the subscapularis and the teres minor. These muscles cover the “ball” of the shoulder (head of the humerus). The muscles work together to lift and rotate the shoulder.
The acromion is the front edge of the shoulder blade. It sits over and in front of the humeral head. As the arm is lifted, the acromion rubs or “impinges” on the surface of the rotator cuff. This causes pain and limits movement.
The pain may be due to a “bursitis” or inflammation of the bursa overlying the rotator cuff or a “tendonitis” of the cuff itself. In some circumstances, a partial tear of the rotator cuff may cause impingement pain.
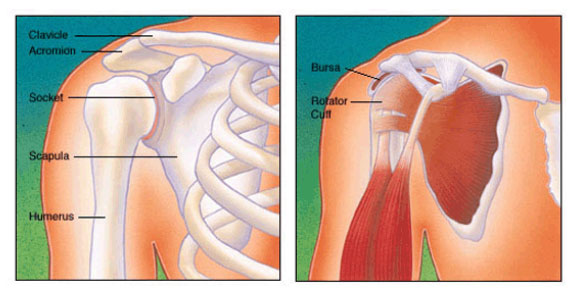
FIGURE 1 – Normal anatomy of the shoulder
Risk Factors/Prevention
Impingement is common in both young athletes and middle-aged people. Young athletes who use their arms overhead for swimming, baseball and tennis are particularly vulnerable. Those who do repetitive lifting or overhead activities using the arm such as paper hanging, construction or painting are also susceptible. Pain may also develop as the result of minor trauma or spontaneously with no apparent cause.
Symptoms
Beginning symptoms may be mild. Patients frequently do not seek treatment at an early stage.
- You may first be aware of minor pain that’s present both with activity and at rest.
- You may have pain radiating from the front of the shoulder to the side of the arm.
- You may note sudden pain with lifting and reaching movement.
- Athletes in overhead sports may have pain when throwing or serving a tennis ball.
Impingement commonly causes local swelling and tenderness in the front of the shoulder. There may be pain and stiffness when you attempt to lift your arm. There may also be pain when you lower the arm from an elevated position.
As the problem progresses, you may have pain at night. You may loose strength and motion. You may have difficulty with activities that place the arm behind the back, such as buttoning or zippering. In advanced cases, loss of motion may progress to a “frozen shoulder”. In acute bursitis, the shoulder may be severely tender. All movement may be limited and painful.
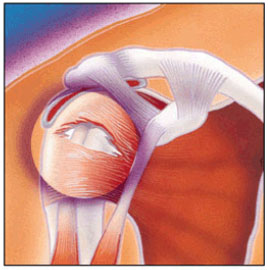
FIGURE 2 – Rotator Cuff Tear
Diagnosis
To diagnose shoulder impingement, an orthopaedic surgeon reviews the symptoms and physically examines
the shoulder.
He or she may take X-Rays. A special X-Ray view called an “outlet view” sometimes will show a small bone spur on the front edge of the acromion (see Figures 3a and 3b). The doctor may request further imaging studies, such as an MRI (magnetic resonance imaging). These can show fluid or inflammation in the bursa and rotator cuff. In some cases, partial tearing of the rotator cuff will be identified.

FIGURE 3A (a normal outlet view x-ray) and 3B (Abnormal outlet view showing a large anterior spur felt to cause impingement on the rotator cuff.
An impingement test, injection of local anesthetic into the bursa, can help to confirm the diagnosis.
Treatment Options
Initial treatment is conservative. The doctor may suggest that you rest and avoid overhead ctivities. He or she might prescribe a course of oral non-steroidal anti-inflammatory medication. Stretching exercises to improve range of motion in a stiff shoulder will also help.
Many patients benefit from injection of local anesthetic and a cortisone preparation to the affected area. The doctor might also recommend a program of supervised physical therapy. Treatment may take several weeks to months. Many patients experience a gradual improvement and return to function.
Treatment Options: Surgical
When conservative treatment does not relieve pain, the doctor may recommend surgery. The goal of surgery is to remove the impingement and create more space for the rotator cuff. This allows the humeral head to move freely in the subacromial space and to lift the arm without pain. The most common surgical treatment is subacromial decompression or anterior acromioplasty. This may be performed by either arthroscopic or open techniques:
Arthroscopic Technique: In an arthroscopic procedure, two ro three small puncture wounds are made. The joint is examined through a fiberoptic scope connected to a television camera. Small instruments are used to remove bone and soft tissue.
Open Technique: Open surgery requires placement of a small incision in the front of the shoulder. This allows for direct visualisation of the acromion and rotator cuff. In most cases the front (anterior) edge of the acromion is removed along with some of the bursal tissue. The surgeon may also treat other conditions present in the shoulder at the time of impingement surgery. These can include acromioclavicular arthritis, biceps tendonitis or a partial rotator cuff tear.
Rehabilitation: After surgery, the arm may be placed in a sling for a short period of time. This allows for early healing. As soon as you are comfortable, you may remove the sling and begin exercise and use of the arm. The surgeon will provide a rehabilitation program based on your needs and the findings of surgery. This will include exercises to regain range of motion of the shoulder and strength of the arm. It may take two to four months to achieve complete relief of pain.